Introduction
Iatrogenic unilateral vocal cord paralysis (UVCP) has emerged as a notable complication following cardiac surgical procedures. It is important to document the recovery and risk of UVCP to quantify the predictors and outcomes. This study aimed to assess the previously inadequately characterized independent predictors and prevalence of UVCP in patients undergoing cardiac surgery; and evaluate the symptom burden and the natural progression of this condition.
Methods
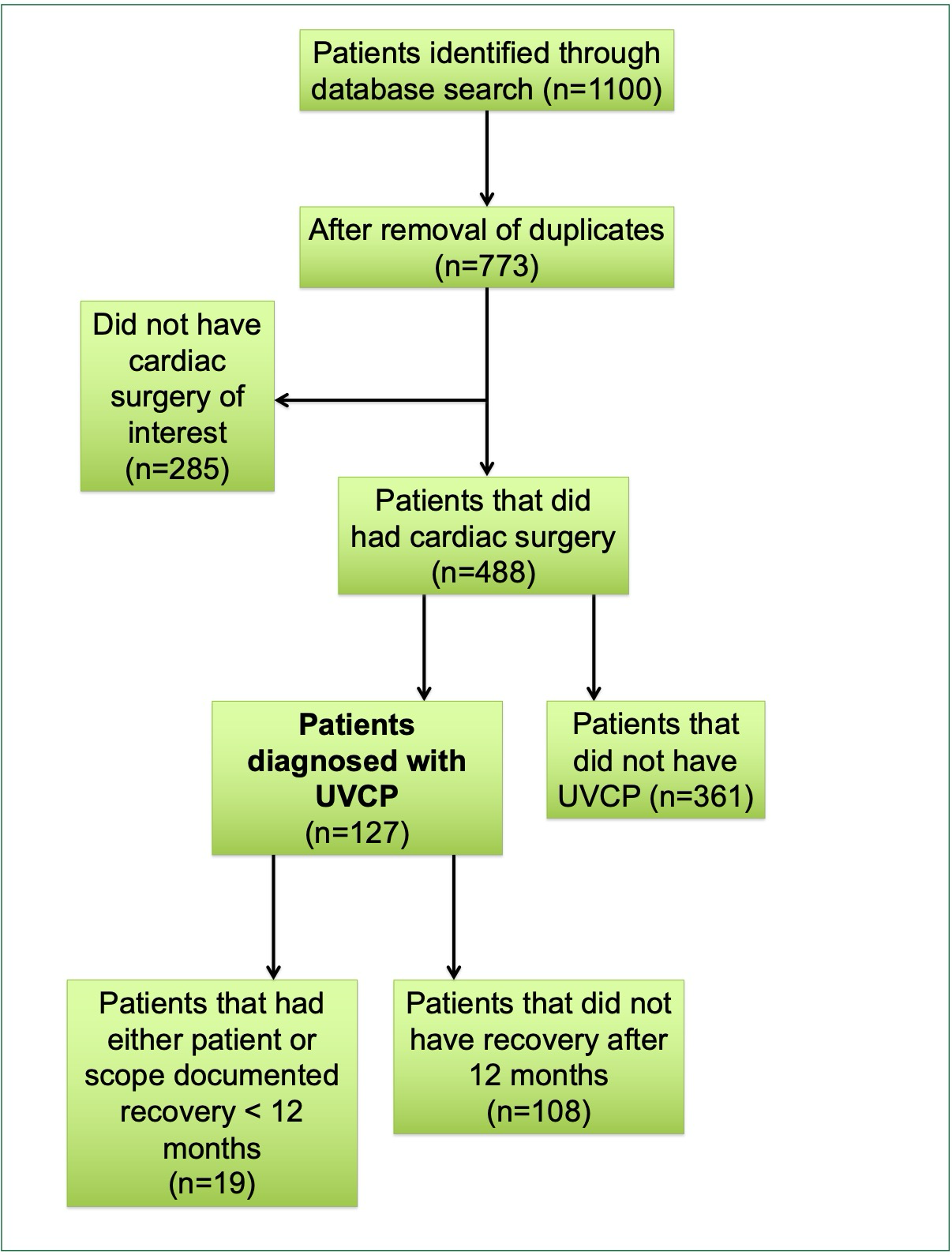
This study employed a retrospective cohort design, focusing on patients who underwent cardiac surgery (n=488) involving manipulation of the aortic arch at the Stollery Children’s Hospital from 2013 to 2023. Patients with UVCP were diagnosed by a pediatric otolaryngologist with fellowship training, utilizing flexible fiberoptic awake laryngoscopy. Children with other diagnoses affecting laryngeal mobility were excluded. Cardiac procedure information, patient demographics, symptom burden, and laryngeal interventions were collected. The association of various factors with UVCP was evaluated using chi-squared, Fisher’s exact, and t-tests. Binary logistic regression analysis was used to identify independent predictors of UVCP.
Results
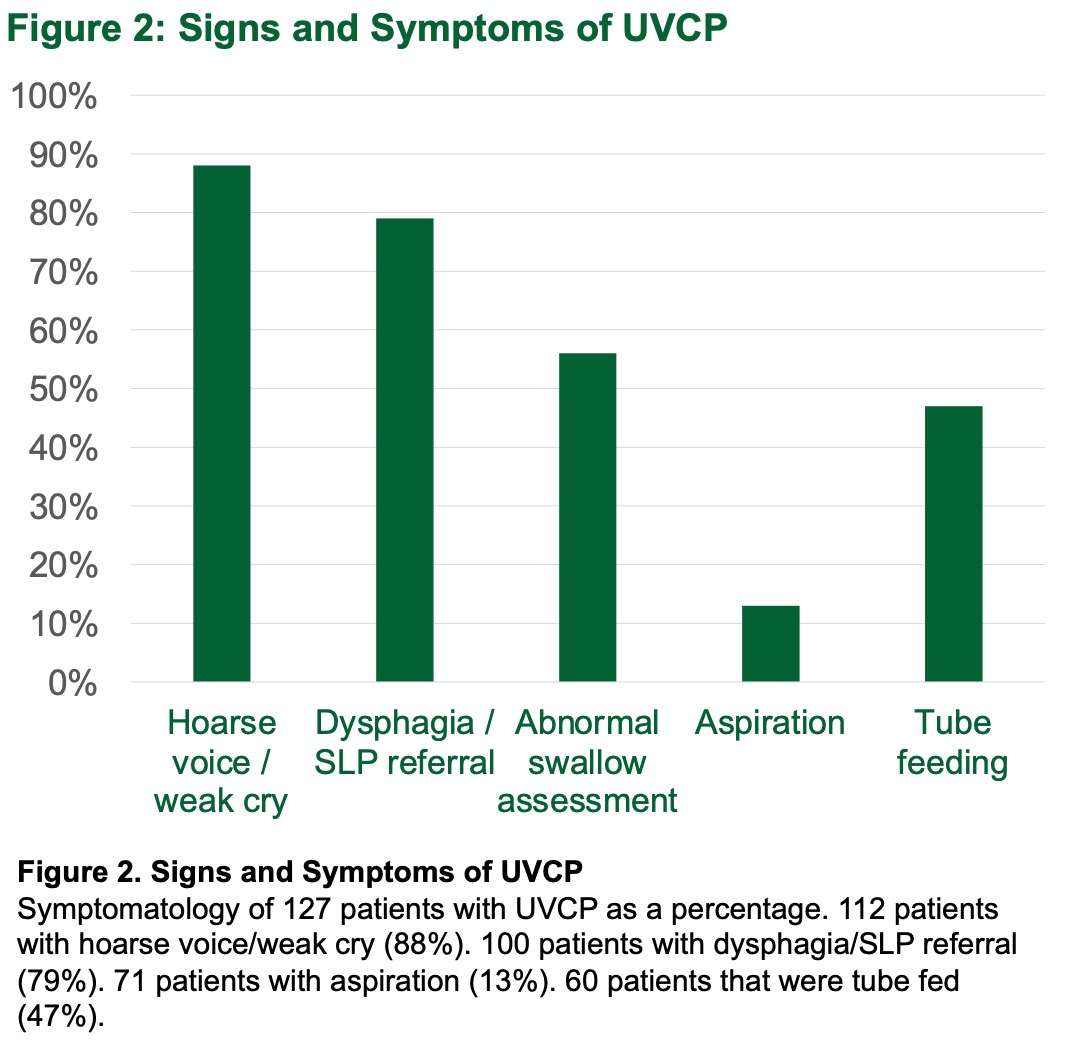
On univariate analysis, PDA ligation as a single procedure (p=0.024), aortic coarctation alone or combined with other cardiac procedures (p=0.006), Norwood procedures alone (p<0.001), interrupted aortic arch repair alone (p=0.024), and having multiple cardiac surgeries (p=0.006) were all found to be significantly associated with UVCP. In total only 31 of the UVCP patients (n=119) had documentation of parent-reported symptom resolution.
Conclusion
The preliminary data suggests that UVCP is common following cardiac surgery, with a significant number of patients experiencing symptoms that persist for over a year. These symptoms are associated with extreme prematurity and specific surgeries are associated with an increased risk of developing UVCP. Further longitudinal prospective studies are required to assess the natural history and to identify management strategies.